By: Emily Westphal, DVM, Diplomate, ACVIM (Cardiology)
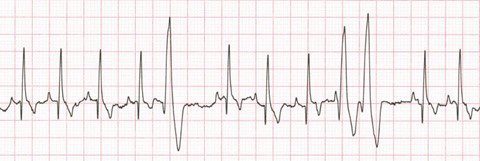
We first met Bella Luna in May of 2019 as an emergency consultation. She collapsed once a home, and again while getting radiographs taken with her primary care veterinarian, Dr. Corbett. An arrhythmia was noted during Dr. Corbett’s physical exam, and she was referred to the emergency service. On presentation to the ER, she had a wide complex tachycardia consistent with ventricular tachycardia, which fortunately converted back to sinus rhythm while her dose of Lidocaine was being drawn up. A cardiac evaluation through CVCA was advised, and an echocardiogram was performed to further define her heart disease. Her echo showed minimal changes to her heart size and function, with these changes presumed to be due to secondary to her recent tachycardia.
Given Bella’s breed and type of arrhythmia with minimal structural heart changes, she was diagnosed with Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC). ARVC is a genetic disease found mainly in Boxer dogs, bulldogs, and rarely cats, in which the normal myocardium is replaced by fatty or fibrofatty tissue, most commonly in the right ventricle. Biopsy is required for definitive diagnosis, but since the disease tends to affect the epicardium first, this is rarely pursued or necessary for treatment. A genetic test is also available through the great work by Dr. Kate Meurs at NCSU. This tests for a mutation in the striatin gene that has been shown to be associated with ARVC in Boxers, although being positive for one or both copies of the mutation does not necessarily mean that the individual dog will end up with the disease. Dogs that carry two copies of the mutated gene (homozygous positive) are more likely to have a severe form of the disease and breeding these dogs may not be recommended.

Since ARVC is a disease primarily of the electrical activity of the heart, 24-hour Holter monitors are key for diagnosis and treatment monitoring. Annual Holter monitors are recommended for screening starting at 3 years of age in Boxer dogs given the high prevalence of disease. ARVC typically causes ventricular arrhythmias with a variable degree of severity ranging from a low number of singlet ventricular premature complexes (VPCs) to sustained runs of ventricular tachycardia which can lead to syncope or sudden death. Supraventricular arrhythmias are also possible. If arrhythmias are severe enough or syncope is present, treatment with antiarrhythmic therapy is recommended.
Like many dogs with ARVC, Bella was treated with Sotalol as her first line antiarrhythmic. She has only had one additional syncopal episode since starting medication almost 2.5 years ago! Bella returns to CVCA every 6-9 months for follow up echocardiograms and Holter monitors to monitor her rhythm and to assess for decrease in heart function which can happen in a small number of cases. Several adjustments to her medications have been made over the years since she was diagnosed, but she continues to live a happy and healthy life thanks to the vigilant care of her family and the quick action of Dr. Corbett.